Introduction
Carbon dioxide (CO2) levels are integral values in the NICU as they relate to cerebral blood flow and titrated respiratory care. High, low, and fluctuating levels of CO2 have been associated with intraventricular hemorrhage (IVH)1 which has been shown to occur in as many as 42% of neonates weighing less than 1500 grams.2 Hypocapnia has also associated with periventricular leukomalacia (PVL)2, permanent white matter damage that is most associated with poor neurodevelopmental outcomes.
While ventilation is key to maintaining CO2 values appropriate for managing IVH and PVL risk (and supporting the underdeveloped lungs of premature infants), mechanical ventilation has been linked to the development of chronic lung disease (bronchopulmonary dysplasia, BPD), which occurs in 40-50% of neonates born below a gestational age of 28 weeks.3
In recent years, to combat the high incidence of BPD, emphasis has been placed on lung protective strategies and gentle ventilation in the NICU. Execution of a lung protecting strategy means ensuring that the respiratory support is sufficient to keep the lung inflated (to avoid derecruitment and atelectasis) but gentle enough to avoid overdistension (and associated volutrauma) while also preventing brain injury. Carbon dioxide levels help guide this titration.
Complexities with Blood Gases and Capnography
Historically, CO2 levels have been available through blood draws, either arterial blood gases (ABGs) or capillary heel sticks (CBGs). While this methodology is considered the gold standard, heel sticks specifically introduce risks associated with pain, infection, and blood loss. The study of long-term impact of neonatal pain is a rapidly growing field with early results suggesting connections between cumulative pain in the NICU and brain formation changes, which are then linked to poorer behavioral and cognitive outcomes even at school age.4-5 Outcomes like these have driven the vast majority of NICUs to employ strategies like clustered care and touch times to lessen the amount (or at least the frequency) of stimulation and pain for their patients. Iatrogenic blood loss has also been a focus of recent research,6 with an emphasis on reducing neonatal anemia as well as transfusion rates.
Intermittent blood gases are additionally limited in the management of neonatal care because the values only represent a moment in time and cannot provide instantaneous results. Often, the blood draw itself causes the patient to react to the pain with crying and stress, likely resulting in their CO2 levels being different from when the sample was drawn.
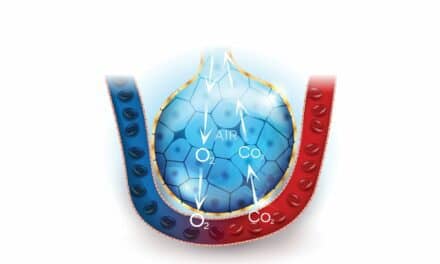
Capnography (end tidal CO2), while continuous, provides little clinical utility in the NICU as the technology is largely inaccurate with small tidal volumes and uncuffed endotracheal tubes, adds deadspace to the ventilator circuit, and is not compatible with high frequency or noninvasive ventilation methods prioritized for neonatal patients. The limitations of both blood gases and capnography make transcutaneous monitoring (TCM) of CO2 a desirable option for patient management in the NICU.
Our Facility’s Experience
Early TCM Experience
Transcutaneous monitoring was first implemented at Hershey Medical Center’s NICU prior to 2009 with limited success. Early challenges were multifaceted: changes in care and technology were difficult to implement across a wide group; concerns about skin integrity or burns remained from team members who had used older iterations of the technology; clinicians at all levels struggled to trust the transcutaneous CO2 (TcPCO2) values and had different opinions about patient selection and implementation; and the maintenance of the devices seemed confusing and overwhelming. Thus, use of the technology was paused.
Implementation Strategy
Because there were still several physicians who believed in the benefits of the technology, our team decided to make a final effort to standardize use and thoroughly evaluate the clinical utility of the technology and equipment. We developed standardized training in conjunction with the manufacturer (Sentec Digital Monitor, Sentec, Therwil, Switzerland), began collecting and analyzing our own correlation data, and organized a proactive approach to device maintenance including roles and responsibilities.
Results
The standardized education program successfully drove competency about the technology, how to use it and maintain the devices, and how the parameters supported our care goals. The correlation data built trust in the transcutaneous values and furthermore allowed our team to identify best practices and develop a deeper understanding of device functionality and optimal use. Clear roles and responsibilities relative to the equipment and the parameter have drastically reduced previous troubleshooting and maintenance issues, and our team is better prepared to handle any issues when they do occur.
Current Clinical Use
Once broad competency was achieved, we quickly expanded the number of transcutaneous monitors from three to nine and then to 16, representing nearly 30% of our licensed NICU beds. Blood gases that were previously performed every four hours were reduced to every 12 hours once a stable trend was achieved for TcPCO2. Blood gases now are obtained once a day, to once or twice per week, or not done at all in the absence of a clinical concern or discrepant TcPCO2 value or trend. TcPCO2 readings and their correlation with blood gases are communicated during rounds, and we have consistently expanded patient selection for transcutaneous monitoring from only patients on high frequency ventilation to any intubated patient, including high frequency oscillatory ventilated patients in the pediatric intensive care unit (PICU). TCM has also been used to monitor patients receiving bubble CPAP to evaluate changes in ventilation status post-extubation.
Enduring Challenges
As with other technologies, extremely low birth weight (ELBW) infants are difficult to manage. Adhesion of the attachment rings is challenging in high humidity environments and with ELBW infants with immature skin. For those babies born <750 grams, finding the appropriate anatomical surface for sensor placement can also be a struggle. Importantly, we have seen the benefit of having continuous TcpCO2 information for these micropreemies and have not had any skin integrity issues related to adhesion or heat from the transcutaneous sensor in this vulnerable population.
Perfusion at the monitoring site and correlation of the TCM are intimately related – therefore any neonate or infant with systemic poor perfusion, low blood pressures, or even a large patent ductus arteriosus (PDA) can present correlation challenges. In these cases, we continue to monitor these patients but rely more on TcPCO2 trends rather than actual values.
Additional Benefits
- Noninvasive, continuous trending values support decision making related to ventilatory management decisions.
- When surveyed, >95% of our providers agree that the use of transcutaneous monitoring reduced the frequency of ordering invasive blood tests, which has implications for outcomes as well as cost.
- Reduction in blood draws was also perceived to have a positive impact on parental satisfaction due to decreased painful stimuli.
Keys to Successful Implementation of the TCM Program
- Develop a training program that addresses all members of the neonatal team: nurses, respiratory therapists, neonatal nurse practitioners, and neonatologists.
- Drive a high level of competency about the relationship between perfusion, device calibration, site selection, and correlation.
- Build broad trust in the technology by generating quality correlation data at the bedside with a review of proper blood sampling technique, and attention to detail with logging TcPCO2 values at the moment the blood draw is performed.
- Establish “super users” and a proactive maintenance strategy to ensure monitors are always ready for use and to minimize time spent troubleshooting.
- Educate the entire team regarding the potential impact of fewer blood draws in relation to blood loss, pain, and infection, as well as the lung protective value of titrated ventilatory care.
Conclusion
With time, effort, and the right education, transcutaneous monitoring can offer neonatal intensive care teams continuous, clinically useful CO2 values that support real-time ventilatory decision-making while reducing the pain, stimulation, and blood loss associated with frequent blood draws.7
RT
Ann Donnelly MS, RRT-NPS, and Jennifer Erkinger MS, RRT-NPS, AE-C, C-NPT, are NICU clinicians at Milton S. Hershey Medical Center, Penn State Health (Hershey, PA).
References
- Hochwald et al. Continuous Noninvasive Carbon Dioxide Monitoring in Neonates: From Theory to Standard of Care. Pediatrics. 2019;144(1):e20183640. doi:10.1542/peds.2018-3640
- Ahn et al. Intraventricular Hemorrhage and Post Hemorrhagic Hydrocephalus among Very-Low-Birth-Weight Infants in Korea. J Korean Med Sci. 2015;30 Suppl 1(Suppl 1):S52-S58. doi:10.3346/jkms.2015.30.S1.S52
- Stoll et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993-2012. JAMA. 2015;314(10):1039-1051. doi:10.1001/jama.2015.10244
- Doesburg et al. Neonatal pain-related stress, functional cortical activity and visual-perceptual abilities in school-age children born at extremely low gestational age. Pain. 2013;154(10):1946-1952. doi: 10.1016/j.pain.2013.04.009
- Chau et al. Hippocampus, Amygdala, and Thalamus Volumes in Very Preterm Children at 8 Years: Neonatal Pain and Genetic Variation. Front Behav Neurosci. 2019;13:51. doi: 10.3389/fnbeh.2019.00051
- Counsilman et al. J Matern Fetal Neonatal Med. 2019 Oct 6:1-6.
- Mukhopadhyay et al. Neonatal Transcutaneous Carbon Dioxide Monitoring–Effect on Clinical Management and Outcomes. Respir Care. 2016 Jan;61(1):90-7. doi: 10.4187/respcare.04212