 |
Oxygen is carried by hemoglobin in the erythrocyte and is also dissolved in the plasma. The most significant portion, oxyhemoglobin, is responsible for 99% of the blood’s oxygen delivery to tissues and cells. The accurate measurement of total hemoglobin concentration, therefore, has a major clinical impact through patient assessment and through the evaluation of therapies that affect cardiopulmonary dynamics.1
Calculated indices used for similar monitoring of oxyhemoglobin saturation and oxygen content also derive their clinical utility from precise total hemoglobin measurements. The accuracy of the total hemoglobin result is a crucial driver of diagnoses, patient-care protocols, and therapeutic interventions. For 2 decades, point-of-care devices have been available to monitor these parameters at the bedside; however, the limitations of sensor technology remain poorly understood, as do the generation of physiologic formulas and the distinction between calculated and measured values. Knowledge of how point-of-care devices analyze and report total hemoglobin, oxyhemoglobin saturation, and oxygen content is essential to prevent misinterpretation of results and ensure patient safety.
Hemoglobin
The majority of point-of-care blood-gas instruments calculate total hemoglobin based on a measured hematocrit.2,3 The reliability of the total hemoglobin value depends on the variables contained in the formula and the accuracy of the hematocrit sensor. Mean corpuscular hemoglobin concentration is first estimated by dividing the hemoglobin by the hematocrit. This is multiplied by the % hematocrit and then divided by 100 to equal total hemoglobin. A normal value for mean corpuscular hemoglobin concentration is 32 to 36 g/dL.
The methodology employed by point-of-care instruments to measure hematocrit is called conductimetry. These hematocrit sensors use the principles that whole blood can conduct an electrical current and that this signal can be calibrated to reflect the hematocrit concentration. The plasma, rich in electrolytes, can conduct an electrical current, but the blood cells, erythrocytes, leukocytes, and platelets have a nonconductive coating that surrounds their outer membranes and prevents their participation in the electrical transmission. Because of their nonconducting properties, blood cells impede the electrical signal. Reduced conduction implies an increase in the number of nonconductive cells; conversely, the greater the electrical conduction, the fewer the blood cells in the sample.
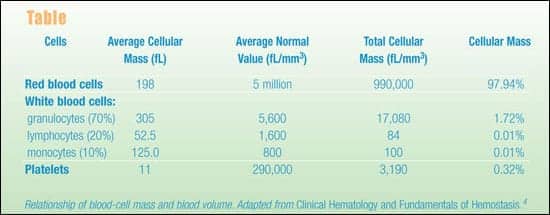
Hematocrit is the percentage of erythrocytes measured in a whole-blood sample. Because the red blood cell contributes to approximately 98% of all nonconducting mass in a whole-blood sample, conductimetry sensors interpret changes in signal transmission as changes in erythrocyte number, or hematocrit concentration (see Table).
 |
The conductive method for hematocrit measurement is robust under normal physiological conditions, but therapies that significantly alter the specimen’s osmolarity can produce a bias. Manufacturers of point-of-care instruments use normal donors’ whole blood to calibrate conductive hematocrit sensors. Some clinical interventions, however, produce significant hemodilution with hyperosmolar solutions, causing conductive hematocrit sensors to understate hematocrit concentration. This can occur during cardiopulmonary bypass or extracorporeal membrane oxygenation procedures when pump-priming solutions are mixed with the patient’s systemic blood volume, as well as during the use of fluid-resuscitation protocols for trauma victims. Another area of concern is the administration of radiographic contrast media for vascular imaging. The osmolarity of these solutions can range from 660 to more than 2,000 mOsm/L. Although a bolus infusion of these agents does not cause the relative hemodilution effects seen in cardiopulmonary bypass, the contrast medium does alter the conductivity of blood.5 Therefore, it has the potential to produce an inaccurate reflection of the patient’s hematocrit, if this is measured using conductimetry.
Typical adult cardiopulmonary-bypass procedures can dilute circulating blood volume in a ratio of 0.3:16, significantly reducing hematocrit and oxygen transport. This (and hyperosmolar solutions administered for other reasons) can increase the conduction properties of the blood beyond the sensors’ calibration specifications. In addition, hyperosmolar effects on red blood cells decrease their mass, adding to the intensity of the electrical signal. This combination erroneously reduces hematocrit measurements. Compounding the hemodilution effect, some protocols add proteins (such as albumin) to the solutions used. Proteins are similar to blood cells in that they do not conduct an electrical current, so this contributes to the distortion of the signal. If these phenomena are not accounted for, the total hemoglobin calculation produced from the hematocrit measurement could be misinterpreted, leading to false interventions and diagnoses. Some manufacturers of point-of-care instruments provide custom correlation adjustments to circumvent this issue.2
Oxyhemoglobin Saturation
Within the hemoglobin molecule, four heme rings composed of ferrous iron are embedded into their own polypeptide chains, of which the protein portions are called globin. Each heme ring can bind one oxygen molecule. Therefore, one hemoglobin molecule can be 0%, 25%, 50%, 75%, or 100% saturated. Each erythrocyte contains approximately 280 million molecules of hemoglobin. Given an average of 5 million red blood cells per mm3 each cubic millimeter of whole blood contains 14×1017 molecules of hemoglobin. The combined average saturation of all oxyhemoglobin can be any value ranging from 0% to 100%.
Not all molecules of hemoglobin carry oxygen. Some hemoglobin binds a hydrogen ion and contributes to base buffering power. This normal form of hemoglobin, reduced hemoglobin, increases proportionally as oxygen is liberated to the mitochondria and hydrogen ions are formed in response to aerobic metabolism. Other derivatives of hemoglobin can develop significant physiological manifestations, often producing marked hypoxia.1 Among these types are carboxyhemoglobin and methemoglobin.
Carboxyhemoglobin forms when hemoglobin is exposed to carbon monoxide gas inhaled into the lungs. Carbon monoxide is a common pollutant in tobacco smoke that affects both smokers and those exposed to secondhand smoke.7 Poorly vented furnaces and smoke inhalation from fires or smoldering carbon-based fuels add to carbon monoxide toxicity.8 The affinity of carbon monoxide for hemoglobin is approximately 210 times stronger than that of oxygen9 and, consequently, the physiological effects of carboxyhemoglobin can be profound. Although the signs and symptoms of anemic hypoxia from elevated carboxyhemoglobin can be severe, measurement of PaO2 often fails to aid diagnosis. Carbon monoxide poisoning is a hemoglobin-based manifestation, and the measurement of oxygen dissolved in the plasma will not detect the presence of this hemoglobin derivative.
Methemoglobin is produced when the ferrous iron contained within the heme ring of the hemoglobin molecule is oxidized to the ferric form of iron. Causes include metabolism of inhaled nitric oxide,10 long-term exposure to high nitrate levels in food and water,11 enzyme deficiencies,12 immature gut development in newborns,13 and drug reactions to oxidizing anesthetic agents (such as benzocaine spray).14 Methemoglobin, like carboxyhemoglobin, does not carry oxygen and, as a consequence, diminishes oxygen-carrying capacity. Because methemoglobinemia is a hemoglobin-derivative pathology, PaO2 will not produce diagnostic evidence of methemoglobinemia and may mislead the clinician into underestimating the degree of hypoxia.
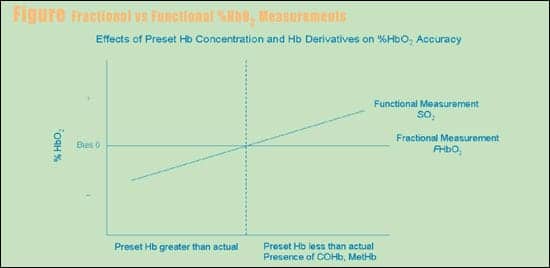
Oxyhemoglobin is first divided by total hemoglobin and then divided by 100 to yield oxyhemoglobin saturation. The oxyhemoglobin saturation formula has been further refined as either a functional or fractional oxyhemoglobin saturation measurement (see Figure). Functional oxyhemoglobin saturation is the result when the total hemoglobin value used in the calculation consists of oxyhemoglobin plus reduced hemoglobin; when carboxyhemoglobin and methemoglobin are also part of total hemoglobin, the result is fractional oxyhemoglobin saturation.
Many point-of-care devices report oxyhemoglobin saturation. Basic blood-gas analyzers calculate this value using algorithms based on an assumed normal oxyhemoglobin dissociation curve and apply a pH variable to fine-tune results. Standard pulse oximeters that use light-emitting diode (LED) wavelengths of 650 and 805 nm have only the capacity to measure oxyhemoglobin and reduced hemoglobin.15 Some whole-blood oximeters, likewise, can measure only functional oxyhemoglobin saturation, with total hemoglobin concentration either preset at the factory or defined by the user.16 When total hemoglobin is overestimated, devices using the functional oxyhemoglobin-saturation methodology will report values that are lower than actual values for oxyhemoglobin saturation. If total hemoglobin is inadvertently underestimated in evaluating patients who have hemoglobin derivatives of carboxyhemoglobin or methemoglobin, functional oxyhemoglobin-saturation calculations will produce a positive bias, compared with fractional analysis.
 |
Oximeters and CO-oximeters use the principle of spectrophotometry to measure the lightwave-absorption characteristics of hemoglobin and its derivatives. While some oximeters only analyze oxyhemoglobin and reduced hemoglobin, others add multiple LEDs to measure the full panel of oxyhemoglobin, reduced hemoglobin, carboxyhemoglobin, and methemoglobin.17 Only CO-oximeters and whole-blood oximeters that analyze all the hemoglobin derivates can measure an accurate total hemoglobin and report a true oxyhemoglobin saturation or fractional oxyhemoglobin saturation. Because spectrophotometry directs its measurement at the individual hemoglobin species, issues of hemodilution and hyperosmolar solutions do not affect readings. This lack of interference makes these point-of-care devices well suited to environments where such fluid-management protocols are common.
Oxygen Content
Oxygen content is the sum of the combined volume of oxygen attached to oxyhemoglobin and oxygen dissolved in the plasma, sampled from a specific anatomic source. Total hemoglobin is multiplied by Hüfner’s number18 and by fractional oxyhemoglobin saturation; the result is then added to the PO2 times 0.003 to yield the oxygen content. Hüfner’s number is the volume of oxygen (in mL) bound by 1 g of hemoglobin. Whether this is 1.34, 1.36, or 1.39 is the subject of academic debate. What is most important is the factor’s consistent use within the institution for trending patient pathology and enacting uniform protocols. All analyzers that calculate oxygen content within the hospital should use the same constant to avoid the misinterpretation of trended results.
The oxyhemoglobin-saturation variable used in the oxygen-content formula can produce significant variance if functional oxyhemoglobin saturation is exchanged for fractional oxyhemoglobin saturation. The Clinical and Laboratory Standards Institute19 (CLSI) stresses that the variables of fractional oxyhemoglobin saturation, total hemoglobin, and PO2 need to derive from the same specimen for clinical accuracy, and that fractional oxyhemoglobin saturation should not be a substitute for a calculated (functional oxyhemoglobin saturation) value.
Most point-of-care oximeters and CO-oximeters do not measure PO2 in their test panels. This omission eliminates the plasma portion of the oxygen-content formula, but the contribution of PO2 is 1% of the total and therefore can be considered negligible, under most clinical circumstances.
Summary
Perfusionists and associated operating-room staff should be knowledgeable in the detection processes used by point-of-care hematocrit sensors, in how conductimetry can report a biased result during cardiopulmonary bypass, and in investigating which instrument features will promote safe patient management. Patients receiving mass volumes of fluids, causing hemodilution with hyperosmolar solutions, can also be found in emergency departments, critical-care units, and cardiac-catheterization suites. RTs, critical-care nurses, medical technologists, and those using point-of-care devices in imaging centers should be mindful of the potential for false hematocrit or total hemoglobin values in these patient-care settings.
In assessing the clinical relevance of results from any laboratory instrument, a clear distinction should be made between measured and calculated values. Similarly, there needs to be an appreciation (and hospital-wide consensus) concerning the clinical circumstances under which calculated results and measured values are not equivalent. Regarding functional oxyhemoglobin-saturation measurements derived by blood-gas instruments, the CLSI standards state, “Clinically significant errors can result from incorporation of such an estimated value for oxygen saturation in further calculations, such as shunt fraction, or by assuming that the value obtained is equivalent to fractional oxyhemoglobin.”20 Calculated values for oxygen saturation reported by blood-gas analyzers and continuous monitoring of peripheral capillary blood using pulse oximetry have clinical utility, but should never be substituted for CO-oximetry in cases of suspected carbon-monoxide toxicity or methemoglobinemia. Direct measurement of oxyhemoglobin saturation and oxygen content is required during right-sided cardiac catheterization procedures for the detection of anatomic shunts. This unique application of oxygen-transport monitoring requires a fractional oxyhemoglobin-saturation analysis to ensure a correct diagnosis and a properly staged severity index.21
The accurate measurement of total hemoglobin is essential to the precise calculation of oxyhemoglobin saturation and oxygen content. These indices of oxygen carrying capacity and transport are vital parameters to monitor in critical-care practice and are available using point-of-care technology. It is of paramount importance for those who conduct point-of-care testing to be trained not only in instrument operation, but in the instruments’ limitations, so that they can avoid erroneous results and inappropriate interventions.
[The preceding two sections were inadvertantly dropped from the print version of this article—Ed.]
Bruce Toben, RRT-NPS, CPFT, is director, clinical affairs and technical solutions, International Technidyne Corp, Edison, NJ. He thanks Diana Blanco, MT, SC (ASCP), for assistance in developing this article’s hematology coverage.
References
- Toben B, Zucker M. Monitoring hypoxia: one step beyond PaO2. Neonatal Intensive Care. 2006;19:27-31.
- IRMA TRUpoint®. Edison, NJ: International Technidyne Corp. Available at www.itcmed.com. Accessed November 2006.
- i-STAT®. East Windsor, NJ: Abbott Point of Care Inc. Available at: www.i-stat.com. Accessed November 2007.
- Harmening DM. Clinical Hematology and Fundamentals of Hemostasis. 4th ed. Philadelphia: F.A. Davis; 2002.
- Steendijk P, Staal E, Jukema JW, Baan J. Hypertonic saline method accurately determines parallel conductance for dual-field conductance catheter. Am J Physiol Heart Circ Physiol. 2001;281:H755-H763.
- Grist G. To wash or not to wash: controlling sodium, glucose and osmolarity in pediatric extracorporeal circuit blood. Available at: [removed]perfline.com/textbook/local/wash_no_wash_ggrist.pdf[/removed]. Accessed November 19, 2007.
- American Lung Association. Smoking and Tobacco. Available at: www.ala.org. Accessed November 2007.
- Harper A, Croft-Baker J. Carbon monoxide poisoning: undetected by both patients and their doctors. Age and Aging. 2004;33:105-109.
- Slonim NB, Hamilton LH. Respiratory Physiology. 3rd ed. St Louis: C.V. Mosby; 1976.
- Taylor MB, Christian KG, Patel N, Churchwell KB. Toxicity of inhaled nitric oxide therapy. Pediatr Crit Care Med. 2001;2:99-101.
- Gupta SK, Gupta RC, Seth AK, Gupta AB, Bassin JK, Gupta A. Methemoglobinemia in areas with high nitrate concentration in drinking water. Natl Med J India. 2000;13:58-65.
- Ash-Bemal R, Wise R, Wright SM. Acquired methemoglobinemia: a retrospective series of 138 cases at two teaching hospitals. Medicine. 2004;83:265-273.
- Sicherer SH. Food protein-induced enterocolitis syndrome: clinical perspectives. J Pediatr Gastroenterol Nutr. 2000;30:S45-S49.
- Nguyen ST, Rafael EC, Bashour CA, et al. Benzocaine-induced methemoglobinemia. Anesth Analg. 2000;90:369.
- Malley WJ. Clinical Blood Gases: Application and Noninvasive Alternatives. Philadelphia: W.B. Saunders; 1990.
- Oxicom®. Rochester, Minn: Waters Medical Systems. Available at www.watrs.com. Accessed November 2007.
- AVOXimeter® 1000E. Edison, NJ: International Technidyne Corp. Available at: www.itcmed.com. Accessed November 2007.
- Hüfner G. Neue versuche zur bestimmung der sauerstoffcapacitat der blutyfarbstoffs. Arch Physiol. 1902;17:130-176.
- National Committee for Clinical Laboratory Standards. Blood gas and ph analysis and related measurements; approved guideline. C46-A. 21:8.
- National Committee for Clinical Laboratory Standards. Blood gas and ph analysis and related measurements; approved guideline. C46-A. 21:7.
- Baim DS. Grossman’s Cardiac Catheterization, Angiography, and Intervention. 7th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.







